
Translate this page into:
Wing denture: A prosthodontic approach to complete dentures for prominent labial ridges
*Corresponding author: Arpit Sikri, Department of Prosthodontics and Crown and Bridge, and Oral Implantology, Bhojia Dental College and Hospital, Budh (Baddi), Solan, Himachal Pradesh, India. arpitsikri@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Sikri A, Kashyap K, Sikri J. Wing denture: A prosthodontic approach to complete dentures for prominent labial ridges. J Adv Dental Pract Res. 2024;3:70-3. doi: 10.25259/JADPR_65_2024
Abstract
Denture teeth and the denture flange are essential components of a complete denture. Ensuring proper labial fullness during fabrication is crucial for aesthetics, but certain cases can be challenging, such as when there is a proclined maxillary anterior ridge or a thick labial cortical plate with significant undercuts. Patients with prominent labial ridges often experience difficulties with conventional dentures, particularly in the maxilla, due to severe undercuts. Traditional complete dentures may compromise aesthetics by creating an excessively thick labial flange. Addressing these issues requires a non-surgical, innovative approach. This case report details a simple, cost-effective, and conservative method for fabricating a denture that enhances facial aesthetics despite the presence of a bulky maxillary ridge.
Keywords
Flangeless denture
Gumfit denture
Labial undercut
Open-faced denture
Prong denture
Window denture

INTRODUCTION
In prosthodontics, ridge anatomy varies significantly among patients, ranging from large to severely resorbed ridges. Achieving proper labial fullness is crucial for the esthetic success of complete dentures.[1] Prominent ridges, particularly in the maxilla, present challenges during denture fabrication, especially in cases involving labially proclined maxillae and associated undercuts. Resorption of the residual alveolar ridge is inevitable, resulting in various ridge morphologies. In severe cases, hard- and soft-tissue undercuts complicate both esthetics and denture fabrication.[2]
While surgical correction may be an option for abnormal ridge conditions, it is not always feasible due to factors such as systemic health issues or lack of patient consent. Although surgical pre-prosthetic procedures can help reduce undercuts, they are not always viable due to medical contraindications or patient reluctance.[3] In these instances, unconventional denture designs, such as prong dentures, can improve aesthetics without the need for surgery. This approach is often referred to as “gum-fit dentures” or “ridge-grip esthetic prostheses.”[4]
Non-surgical solutions, such as flangeless or windowed dentures offer a conservative and cost-effective alternative. This article discusses the fabrication of a wing denture to enhance esthetics for a patient with a bulky maxillary ridge, providing a pleasing and non-invasive solution for such cases.
CASE REPORT
A 60-year-old female housewife from Parwanoo reported to the Department of Prosthodontics, Crown and Bridge, and Oral Implantology at Bhojia Dental College and Hospital in Baddi, Solan, Himachal Pradesh, India, with a chief complaint of missing teeth and difficulty chewing food. She had been edentulous in both the upper and lower arches for the past year, with the primary reason for tooth loss attributed to dental caries. As a new denture wearer, she expressed a need for dentures to restore her ability to chew properly. The patient’s past medical history revealed no significant findings, and her present and personal histories were also unremarkable. She exhibited a philosophical, mental attitude, indicating a balanced approach to her health and dental needs.
On extraoral examination, the patient’s facial form was ovoid, and she displayed an orthognathic facial profile. Her face was bilaterally symmetrical, although a decrease in facial height was observed. Facial muscle tone was normal. She had brown eyes, a medium fair complexion, and thin lips of average length. Examination of the temporomandibular joint revealed normal movements with no significant findings, and lymph nodes were non-palpable.
The evaluation of the residual ridges revealed a U-shaped maxillary arch and a V-shaped mandibular arch. The residual ridge was bulbous with a prominent premaxilla [Figure 1] and a knife-edge anterior mandible, classified as Class III in ridge relation, with adequate interarch distance. A labial undercut was present, but no significant bony irregularities or retained root fragments were found. The mucosa appeared keratinized, and both the lip and cheek mucosa were normal. In the floor of the mouth, the lingual frenum was normal, genial tubercles were not observed, and the retromylohyoid fossa was classified as Type 1. The tongue exhibited keratinized mucosa of normal size with a normal gag reflex. The palate assessment showed a prominent incisive papilla and rugae with normal mucosa. The compressibility of the palate was rigid, and the palatal vault was U-shaped. The junction of the hard and soft palate was classified as Class 1, while the posterior palatal seal area was compressible. The vestibule was shallow in both the maxilla and mandible, with high frenal attachments. Saliva production was mixed and normal.

- Prominent maxillary labial ridge.
Due to financial constraints and a reluctance to undergo surgery, an unconventional complete denture was selected.
Procedure
The fabrication of complete dentures began with primary impressions of the maxillary and mandibular arches using a medium-fusing impression compound (Hiflex Impression Compound, Prevest DenPro Limited, Jammu, India) [Figure 2a]. Beading and boxing of the primary impressions were performed with type II dental plaster (Gyprock Plaster, Rajkot, Gujarat, India) to create proper primary casts [Figure 2b]. A wax spacer was then applied to the primary cast, leading to the fabrication of custom trays using autopolymerizing acrylic resin (DPI RR Cold Cure, Dental Products of India, Mumbai, India). Border molding was executed with low-fusing green stick compound (Pinnacle Tracing Sticks, Dental Products of India, Mumbai, India), and the wax spacers were removed from the individual trays to make final impressions using zinc oxide eugenol wash impression material (DPI Impression Paste, Dental Products of India, Mumbai, India) [Figure 3a]. Beading and boxing of the final impressions were performed to obtain well-formed master casts, which were poured using type III gypsum product, dental stone (Gyprock Stone, Rajkot, Gujarat, India) [Figure 3b]. Afterward, temporary denture bases and occlusal rims were fabricated. Orientation jaw relations were recorded using a facebow (Hanau™ Springbow, Whip Mix, Kentucky, USA) and transferred to a semi-adjustable articulator (Hanau™ Wide-Vue, Whip Mix, Kentucky, USA). Following this, tentative jaw relations were established, and after recording the centric relation, the casts were mounted on the articulator.
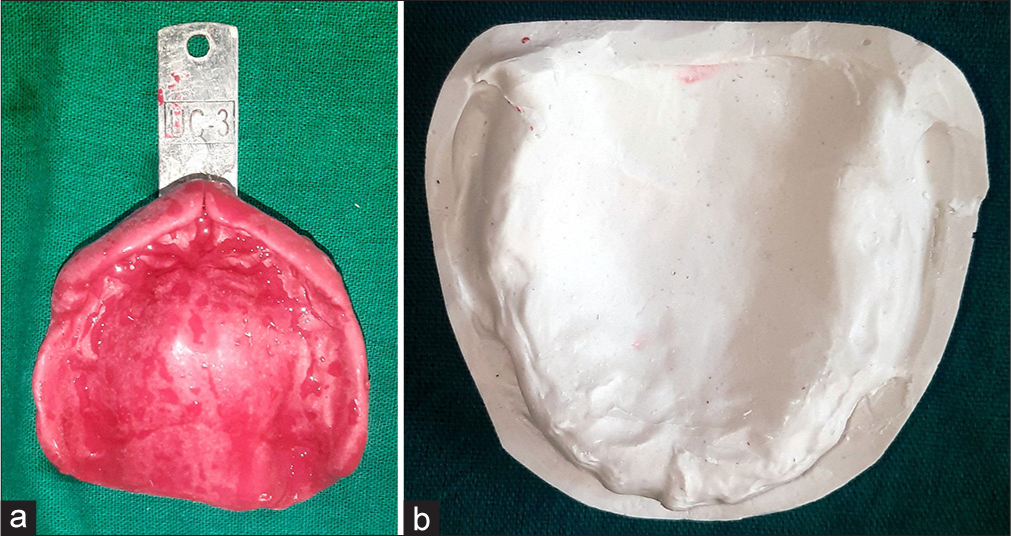
- (a) Maxillary primary impression. (b) Maxillary primary cast.
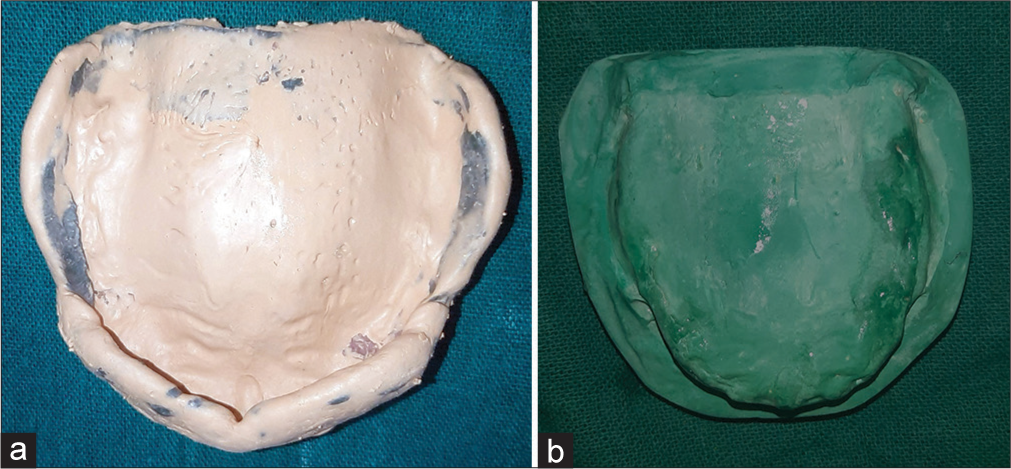
- (a) Maxillary final impression. (b) Maxillary final cast.
Teeth selection and arrangement were conducted according to ideal principles, followed by an intraoral assessment of the waxed-up trial denture to verify function, fit, and esthetics [Figure 4]. The trial denture base was sealed to the definitive casts before de-articulation. The flasking procedure was carried out for both arches and after dewaxing and the application of a tin foil substitute (DPI Heat Cure Cold Mold Seal, Dental Products of India, Mumbai, India), the denture was packed and processed conventionally (DPI Heat Cure, Dental Products of India, Mumbai, India). The processed dentures were cleaned with an ultrasonic cleaner before final insertion. The dentures were polished and tried in the patient’s mouth to evaluate esthetics and occlusion followed by necessary corrections.

- Waxed-up try-in.
The labial flange was removed to create a wing design, reducing labial fullness [Figure 5]. The final wing denture was delivered, and the patient expressed satisfaction with the aesthetics, function, and phonetics during follow-up visits [Figure 6].
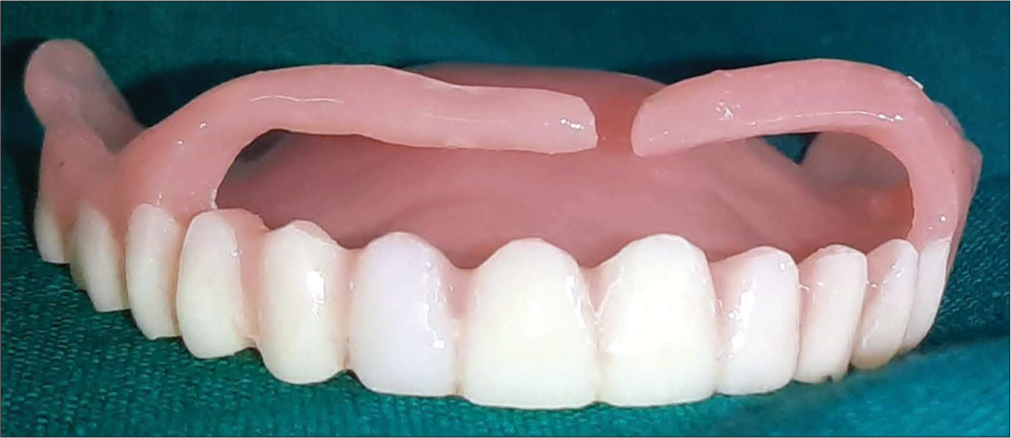
- Wing denture.
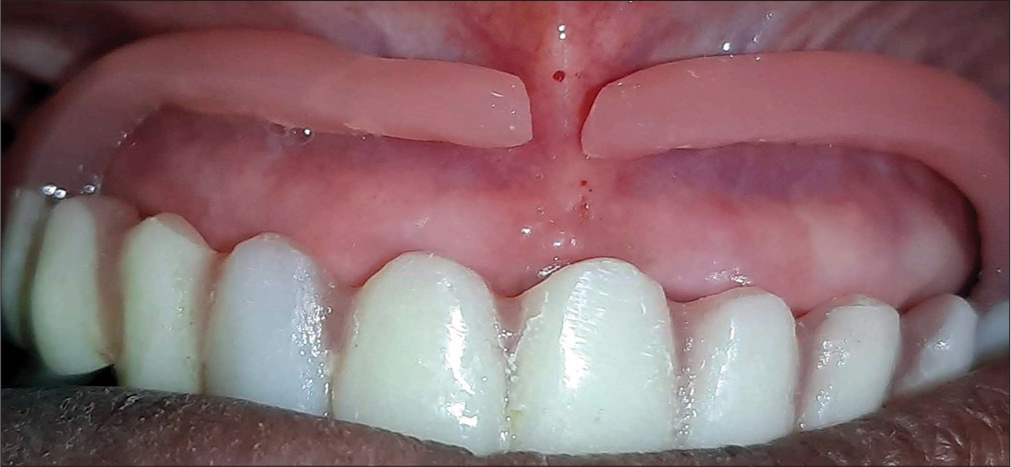
- Wing denture (in patient’s mouth).
DISCUSSION
The flangeless maxillary denture technique provides a preview of the esthetic outcome and is sometimes integrated into the final denture design. These dentures are referred to by various names, including wing denture, ridge grip, or gum fit. In certain cases, a prominent modiolus, particularly with a hypertonic maxillary lip, can reduce the vestibular space unless the labial cortical plate undergoes resorption.[5] Using a conventional denture in such instances can lead to excessive labial fullness, resulting in poor esthetics and phonetic interference.
The “wing denture” modification involves sectioning the labial flange at the frenum region, creating space for the labial frenum while allowing two wings to extend from either side.[6] Accurate diagnosis and treatment planning are crucial for the successful fabrication of complete dentures, especially for patients with prominent maxillary labial ridges.[7] These ridges can result in excessive labial flange thickness, compromising both esthetics and phonetics. In addition, undercuts, particularly hard tissue undercuts, can affect denture retention.[8]
Non-surgical approaches, such as wing dentures, offer conservative options for patients with systemic contraindications to surgery, including uncontrolled diabetes or hypertension.[9] Soft resilient liners can adapt to undercuts without causing trauma to the mucosa.[10] This article discusses the fabrication of a wing denture for a patient with a bulky maxillary ridge and severe labial undercut, ensuring enhanced esthetics without sacrificing functionality.
CONCLUSION
The fabrication of complete dentures should prioritize patient-specific customization to address the unique anatomical and functional challenges presented by each individual. Wing dentures represent a viable alternative for patients with over-contoured maxillary ridges who prefer non-surgical options. These dentures effectively manage the challenges posed by obliterated labial vestibules, often resulting from hypertonic maxillary lips or overactive modiolus muscles, ensuring optimal esthetics and improved patient satisfaction.
This clinical approach demonstrates that wing dentures offer a minimally invasive, cost-effective, and efficient method for rehabilitating proclined maxillary ridges with labial undercuts. The simplicity of the design facilitates ease of insertion and removal, enhancing patient comfort and compliance. Moreover, the non-surgical nature of this technique significantly reduces potential morbidity and post-treatment recovery time, making it a practical solution in the management of edentulous patients with complex ridge anatomy. By combining functionality, esthetics, and patient-centered care, wing dentures contribute meaningfully to the armamentarium of modern prosthodontics.
Ethical approval
Institutional Review Board approval is not required.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Nil.
References
- Effects of complete dentures on facial esthetics. J Prosthet Dent. 1964;14:231-55.
- [CrossRef] [Google Scholar]
- Rehabilitation of the edentulous patient: fabrication of complete dentures In: Zarb G, Bolender C, Carlsson GE, eds. Boucher's prosthodontic treatment for edentulous patients (12th ed). St Louis: Mosby; 2004. p. :209-72.
- [Google Scholar]
- Differences in lip support with and without labial denture flanges in a maxillary edentulous population-Part 2: Blinded subjective analysis of facial esthetics. J Prosthodont. 2018;27:17-21.
- [CrossRef] [Google Scholar]
- How dentition status and masticatory function affect nutrient intake. J Am Dent Assoc. 1998;129:1261-9.
- [CrossRef] [PubMed] [Google Scholar]
- Esthetics for denture patients. J Prosthet Dent. 1980;44:608-15.
- [CrossRef] [PubMed] [Google Scholar]
- A clinically viable index for quantifying denture plaque. Quintessence Int. 1996;27:569-73.
- [Google Scholar]
- Changes in facial form relative to progressive atrophy of the edentulous jaws. Int J Oral Maxillofac Surg. 2004;33:676-82.
- [CrossRef] [PubMed] [Google Scholar]
- Three-dimensional esthetic analysis in treatment planning for implant-supported fixed prosthesis in the edentulous maxilla: Review of the esthetics literature. J Esthet Restor Dent. 2011;23:219-36.
- [CrossRef] [PubMed] [Google Scholar]
- Preprosthetic surgery in elderly. J Prosthet Dent. 1994;72:551-8.
- [CrossRef] [PubMed] [Google Scholar]
- Glossary of prosthodontic terms. J Prosthet Dent. 2005;94:10-92.
- [CrossRef] [PubMed] [Google Scholar]




